Secretory Carcinoma (SC)
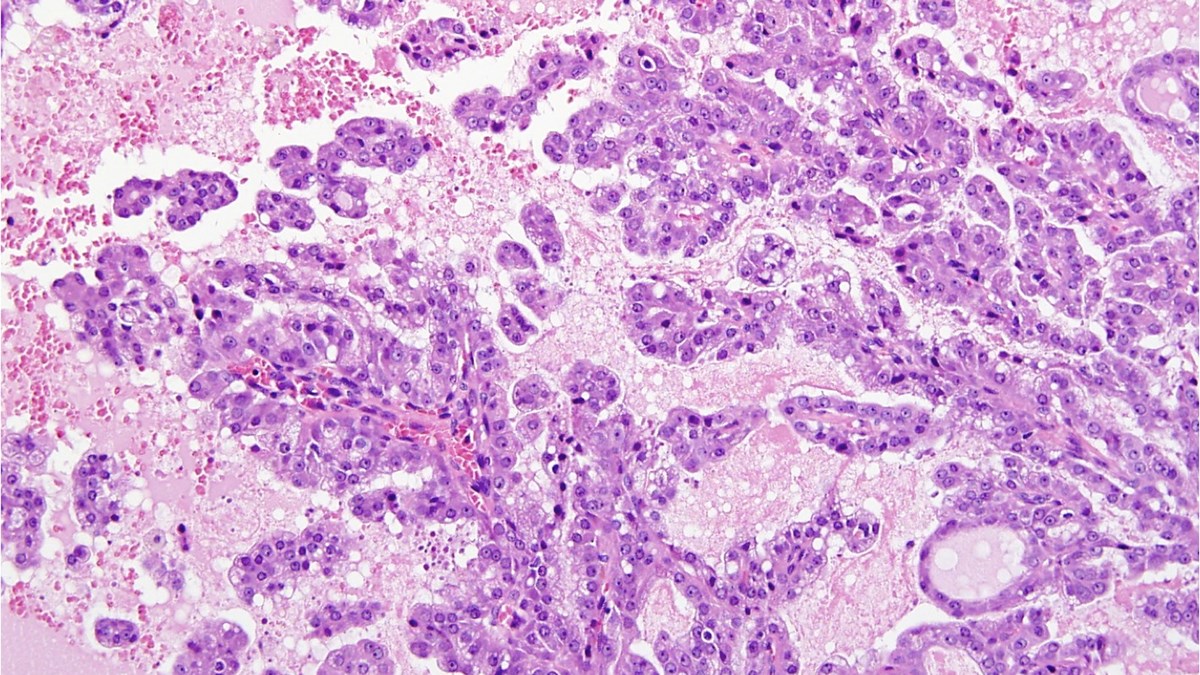
Secretory Carcinoma
Secretory carcinoma (SC) is extremely rare, making up less than 0.3% of all salivary gland cancers. SC usually occurs in people in their 40s to 60s and affects slightly more men than women (1-4). Most SC form in the parotid gland (just below and in front of each ear) with a few cases having been reported in the minor salivary glands (1, 3). Minor salivary glands produce 5% to 8% of saliva and can be found in almost any part of the mouth (4). SC forms a slow-growing, painless lump which is often found by accident (3).
Although a biopsy of the tumour can be used to gather information, in most cases genetic analysis is needed to confirm diagnosis of SC (6, 7). Genetic analysis of SC reveals an unusual rearrangement of chromosomes, producing a fusion of ETV6 and NTRK3 genes (2).
SC is generally considered a less aggressive salivary gland cancer, although occasionally aggressive SC have been reported (5). Most SC have a good long-term outlook and have a low chance of coming back or spreading to other parts of the body (1, 3).
The treatment choice for SC is similar to other salivary gland cancers, and involves surgery to remove the entire cancer, with healthy tissue around it (7). Local radiotherapy is recommended after surgery for patients with large tumours or those at high risk of the tumour coming back (5).
Chemotherapy has been used to treat aggressive SC which has spread to other parts of the body; however, these drugs have shown limited affect (8). Some patients with SC have responded to targeted drugs such as larotrectinib or entrectinib, which has led to these drugs being included in treatment recommendations for health professionals (7).
Useful resources
Read more about how to get your tumour profiled and add to the research biobank at the Christie Hospital in Manchester, UK here:
- Gene profiling or tumour profiling or genomic testing - Salivary Gland Cancer UK
- Donate tissue to the Biobank - Salivary Gland Cancer UK
References
- Langah NA, Ahad A, Ghaloo SK, Faisal M, Hussain RT, Shah FA. Secretory carcinoma of minor salivary glands of buccal mucosa: A case report and review of the literature. Int J Surg Case Rep. 2023;107:108357.
- Boliere C, Murphy J, Qaisi M, Manosca F, Fung H. Mammary Analogue Secretory Carcinoma of the Palate: Case Report and Review of the Literature. Case Rep Dent. 2019;2019:7416302.
- Sethi R, Kozin E, Remenschneider A, Meier J, VanderLaan P, Faquin W, et al. Mammary analogue secretory carcinoma: update on a new diagnosis of salivary gland malignancy. Laryngoscope. 2014;124(1):188-95.
- Ghannam M, Singh P. Anatomy, Head and Neck, Salivary Glands Treasure Island (FL): StatPearls Publishing; [updated 2023 May 29. Available from: https://www.ncbi.nlm.nih.gov/books/NBK538325/.
- Mokhles P, Sadeghipour A, Babaheidarian P, Mohebbi S, Keshtpour Amlashi Z, Gharib MH, et al. Salivary gland secretory carcinoma presenting as a cervical soft tissue mass: a case report. J Med Case Rep. 2024;18(1):78.
- Montalvo N, Galarza D, Redrobán L. Secretory Carcinoma of the Parotid: Making the Correct Diagnosis of a Rare Salivary Gland Carcinoma When Molecular Biology Testing Is Not Available. Case Reports in Pathology. 2019;2019:5103496.
- van Herpen C, Vander Poorten V, Skalova A, Terhaard C, Maroldi R, van Engen A, et al. Salivary gland cancer: ESMO-European Reference Network on Rare Adult Solid Cancers (EURACAN) Clinical Practice Guideline for diagnosis, treatment and follow-up. ESMO Open. 2022;7(6):100602.
- Cipriani NA, Blair EA, Finkle J, Kraninger JL, Straus CM, Villaflor VM, Ginat DT. Salivary Gland Secretory Carcinoma With High-Grade Transformation, CDKN2A/B Loss, Distant Metastasis, and Lack of Sustained Response to Crizotinib. Int J Surg Pathol. 2017;25(7):613-8.
Last Updated April 2024